
Rosacea Acne Treatment Procedures in Singapore

Rosacea is a chronic inflammatory disorder primarily of the facial skin where the causes of it are still unclear. The ‘rash and blushing’ or constant redness happens from excessive dilation of the facial blood vessels triggered by inflammatory pathways in the body. It typically appears with the common symptoms which accompany inflammation, such as burning and stinging sensations, swelling or oedema, and pustules on the skin. There is no permanent cure for rosacea, however, medical therapy is available in Singapore to control or reverse its signs and symptoms.
There are currently several different types of rosacea, as well as multiple triggers of rosacea that have been studied. However, the triggers of rosacea in different individuals may have several unproven theories (e.g. blood vessel abnormalities or large numbers of tiny mites called Demodex Folliculorum on the skin, or bacteria in your gut) which can lead to misinformation or even being treated wrongly for other skin disorders like dermatitis or eczema. Generally, rosacea:
For the classification of rosacea, there are currently 4 different subtypes of this skin condition.

Microscopic examination of the cells of people with ETR shows that there are typically non-specific features, other than the presence of enlarged, dilated, non-lymphatic small blood vessels (capillaries) and veins in the upper and middle parts of the skin layer. These capillaries frequently have bizarre shapes. Assessing the skin cells also shows mild-to-moderate swelling that might not be visible to the naked eye. Inflammation typically occurs throughout all skin layers, with the levels of inflammation changing depending on the trigger. To distinguish ETR, it commonly has:

Inflammatory rosacea includes patients who develop papules or pustules usually over the central regions of the face, hence the word ‘papulopustular’. A papule is a raised area of skin tissue that’s less than 1 centimetre around, and a pustule is a similar form of raised skin except with yellowish fluid inside called pus. They can be usually mistaken as acne, and rosacea used to be known as ‘rosacea acne’ (Read below in ‘What is Rosacea Acne?’). In severe cases, these episodes of inflammation can lead to chronic facial swelling. Other than redness, they are distinguished by:

When it comes to phymatous rosacea, it’s not just about skin redness and blushing. Have you heard of the term ‘strawberry nose’? That is actually a form of phymatous rosacea, called ‘rhinophyma’ (rhino referring to nose). ‘Phymas’ are nodules, swelling, or small, rounded tumours of the skin, hence the term ‘phymatous’ rosacea as nodules can form over the nose, chin, forehead, ears, and eyelids. This form of rosacea happens more often in men and those of European descent, and can usually be distinguished by:

Ocular rosacea can be one of the more difficult forms of rosacea to handle due to the involvement of the eyes. It can cause near constant watering and tearing up during a flare, and can also result in blocked oil ducts of the eyelids that can cause crusting. It is often misdiagnosed in the beginning as an eye infection, leading to a late diagnosis and treatment. They can be distinguished with:
Read More: The Four Types of Rosacea – All About it
‘Diagnostic features’ means the signs that clinicians look out for to diagnose rosacea. The person suffering from rosacea may have major and secondary features or symptoms.
|
Diagnostic Features
|
Major Symptoms
|
Secondary Symptoms
|
|---|---|---|
|
- Persistent Centro-facial erythema (redness) associated with aggravation by trigger factors
- Phymatous changes (Nodules, bumps on the skin with or without pus) |
-Flushing/transient erythema (Redness)
- Inflammatory papules and pustules - Telangiectasia (Visible broken spider veins) - Ocular manifestations (Eyelid telangiectasia, blepharitis, conjunctivitis) |
- Burning sensation
- Stinging sensation - Edema/Swelling - Dry sensation of the skin |
Read More: How To Tell If Your Acne Is Actually Rosacea
Rosacea treatment in Singapore often includes laser treatment procedures or pulsed light therapy. This mainly aims to target very visible blood vessels which contribute to excessive flushing. Laser treatments can work two ways: Using heat to ‘cauterise’ or ‘collapse’ the blood vessels, or using a non-heat version to break up the red patches.
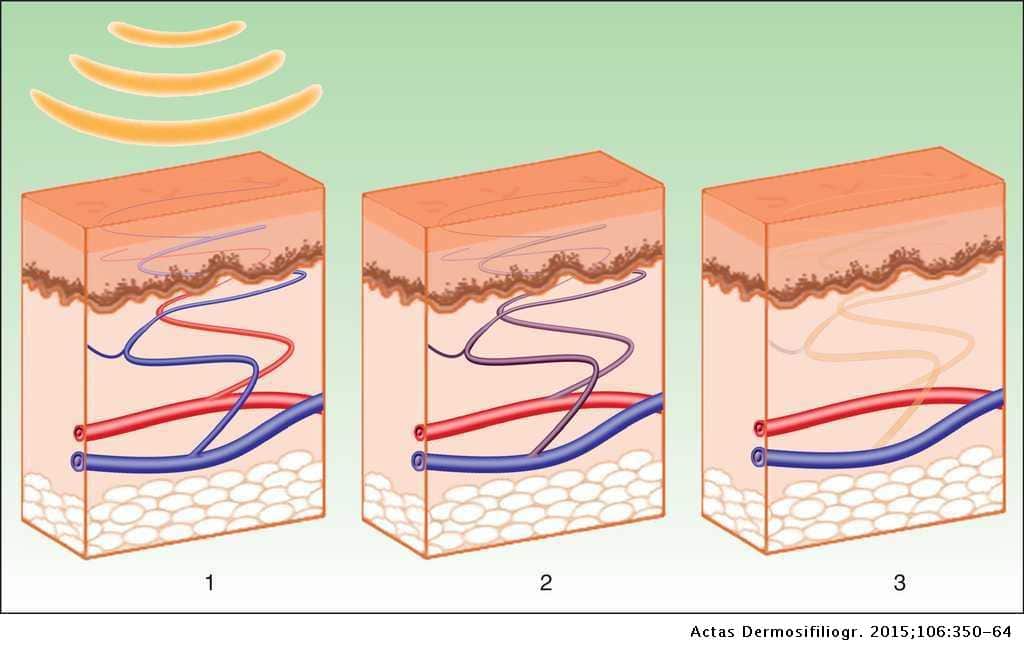
Such lasers can be the Q-switched ND:YAG laser or pulsed laser therapy like the Pico Laser and the Laser, although several sessions over a period of time are needed to see results. Some studies which support the use of laser are:
Some side effects in those studies reported were of hyperpigmentation, a period of rosacea exacerbation, or bruising after the procedure. Hence, the suitability of candidates is important. Very inflamed skin may require the use of oral or topical medication first before undergoing laser therapy to prevent the occurrence of these side effects.
Electrosurgery uses a different method to address the visible blood vessels or excessive tissue growth because of rosacea (phymatous rosacea). This procedure involves the insertion of a very thin needle into the surface of the skin. A carefully selected electric current is used via the needle to target those blood vessels or excess tissue, which respond by clotting (blood coagulation) and shrinking. A scab will form over the treated areas which will eventually fall off on its own, leaving behind a smaller area of previously symptomatic skin.

This method is typically used for rhinophyma, the excessive growth of skin tissue over the nose regions in men who have phymatous rosacea. This is because it can cause scarring, especially when used over larger areas.
A review on the treatment methods available for such symptoms have found that laser treatment usually produces an equal cosmetic result when compared to electrosurgery, making laser a preferred choice due to less risk of scarring.

Dermabrasion does not involve lasers or electric current. Instead, the name dermabrasion is from the combination of ‘dermal’ and ‘abrasion’ – the exfoliation and removal of the superficial layer of your skin through non-surgical methods. Typically, tiny crystals are used to break up the skin cells to reveal the smoother skin underneath. Some patients with rosacea also have very sensitive skin, especially those experiencing the erythematotelangiectatic (ETR) or papulopustular (PPR) subtype of rosacea. Hence, dermabrasion is often used for phymatous rosacea; however, similar to electrosurgery, dermabrasion runs the risk of scarring after the procedure. The dermabrasion acts to ‘sand down’ the upper layers of excessive skin tissue and encourage new and smoother skin cells to replace the area.
Again, it can be said that other more suitable treatment techniques like oral or topical anti-inflammatory medication and the use of laser can provide excellent results with less risk of harmful side effects in rosacea patients. The consultation of a dermatologist is important to identify which treatment works best for you.
Absolutely. Other than the unwanted social effects of feeling embarrassed or frustrated, the physical symptoms of burning, itching, and sensitive skin can be equal causes to treat rosacea. Untreated rosacea can get worse over time because of chronic inflammation of the blood vessels – the skin layer tends to become thinner, more sensitive, and with more visible blood vessels.
We understand that treating rosacea can be a long process to find a treatment that works for you. If you’d like to come in for a consultation on the procedure of rosacea treatment in Singapore to assess if you are suitable for a specific treatment, book an appointment today with SL Aesthetic.
Right at a glance, rosacea tends to look like a tendency to blush easily. When looking at it closer, those red areas may become a persistent and deeper shade of red, with small dilated blood vessels, bumps or scaly skin, or pus-filled spots. During a bad flare, there can be swelling around the red area, especially if the eyes are affected. When phymatous changes happen, nodules tend to grow. Such areas like over the nose or chin can become enlarged, bulbous, and red.
‘Rosacea Acne’ is actually an older term for inflammatory or papulopustular rosacea before the right classifications came along. This is because of the formation of papules or pustules, which take on the look of an acne flare-up. The difference between acne vulgaris (the skin condition where hair follicles become clogged with dead skin and oils resulting in inflammation) and acne rosacea is that rosacea is usually not accompanied by blocked pores or comedones. In a true acne vulgaris condition, there is the presence of blackheads and whiteheads.
Rosacea sufferers have the formation of pimple-like nodules with or without pus, but without the blocked pores; and unlike acne vulgaris which appears anywhere on the face, rosacea is typically localised over the central face (e.g. medial cheek under the eyelids, nose, forehead).
Those who tend to get rosacea acne are women, and most likely with a family history of rosacea although this is not a prerequisite of getting rosacea acne. Individuals who have a more extreme reaction to temperature changes, heat, cold, exercise, UV radiation, and spicy food and alcoholic beverages also tend to be more susceptible to rosacea. They tend to have transient receptor potential channels (TRP channels) in the skin that are more sensitive to ‘inflammatory’ substances like those, which become activated faster hence producing redness. It is less frequent in those with naturally darker skin and is uncommon in children.
Although rosacea seems to run in families, there is no clear genetic link and scientists are still researching theories on how rosacea gets inherited. Overall, more family members with rosacea usually mean a higher risk of inheriting it.
Common triggers of rosacea are:
Unfortunately, yes. Although the causes of rosacea are many and cannot be the same for each person, the tendency is that it gradually worsens with age especially if left untreated. Rosacea is usually manifested as flushing in patients in their 20s, becomes troublesome to patients in their 30s, and may continue to progress thereafter.
No, rosacea is not contagious! You cannot pass on rosacea from one person to another person. This skin condition is not bacteria-led but more of an immune condition, and touching someone with rosacea will not cause that person to develop rosacea.
The National Rosacea Society found that of 1,141 rosacea patients, 55% had suffered from another skin disorder at some point in their lifetime. Commonly reported skin conditions are atopic dermatitis/eczema, scalp dermatitis, and acne vulgaris.
Rosacea flare-ups tend to come and go in cycles. Over time and with the right rosacea treatments that are suitable for your current condition, there can be longer periods between flare-ups, or flare-ups will tend to recover quicker. So while there is unfortunately no cure for rosacea, time, good treatment (such as laser treatment for rosacea in Singapore), and a whole lot of patience can go a long way.
Although allergies in itself cannot 100% cause rosacea in an individual, a strong allergy reaction can trigger a rosacea outbreak. Substances which cause a systemic inflammatory reaction (such as coming into contact with pollen a.k.a. ‘Hayfever’, or going into an old house with plenty of dust mite colonies) can trigger the same inflammatory pathways which are involved in rosacea. It can cause the already sensitive blood vessels in your face to dilate further, bringing a blood rush to those areas, along with stinging, burning, and watery eyes. All this along with the irritation that the allergy itself brings – watery sinuses and sneezing – it is always a good idea to identify your allergens and have medication on hand for the times that it is unavoidable.
While rosacea as a condition cannot be completely prevented, flare-ups can often be controlled well enough. This includes lifestyle changes such as:
Like what you read? Share them!

Not sure if this treatment is right for you? Speak with our team in a no-obligation consultation, and view real patient results.

